When a patient hears that an implant is possible, but only after bone reconstruction, the next question is almost always practical: how many surgeries, how long will it take, and can the result be trusted? That is exactly what the query “восстановление кости перед имплантацией этапы лечения” is really about – not just bone volume, but predictability.
In implant dentistry, bone loss is common. It may happen after a tooth has been missing for years, after infection, after trauma, or simply because the upper jaw near the sinus does not offer enough height for stable implant placement. The good news is that lack of bone does not automatically mean lack of options. The important part is choosing the right sequence of treatment, because the stages are not identical for every patient.
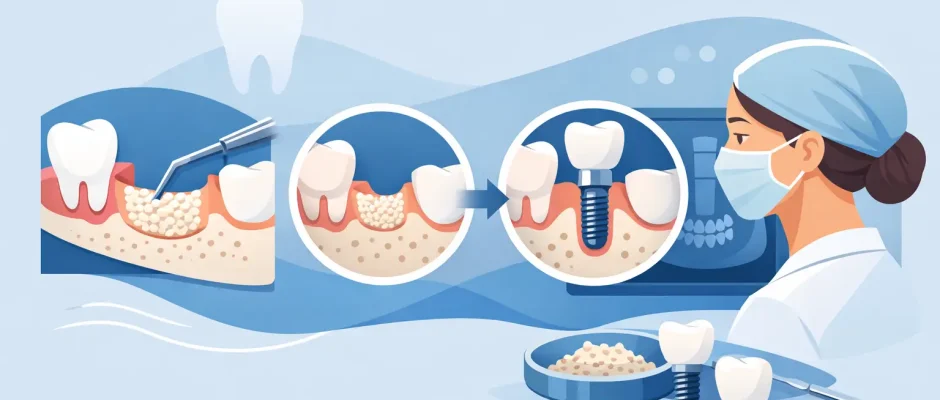
Bone grafting before implants: treatment stages
The first stage is not surgery. It is diagnosis. A proper treatment plan starts with clinical examination and a CBCT scan, not with a guess based on a regular dental X-ray. Three-dimensional imaging shows the true width and height of the bone, the position of the sinus or nerve, the quality of the tissue, and whether an implant can be placed immediately or only after augmentation.
This stage also defines the cause of the defect. A small loss after a recent extraction is very different from severe long-term atrophy. A socket with an active infection is different from a healed ridge. In some patients, the missing volume is horizontal – the ridge is too thin. In others, the problem is vertical – there is not enough height. Sometimes both are present. That distinction matters because it changes the technique, the healing time, and the level of surgical complexity.
Stage 1: planning and risk assessment
A careful plan includes more than measuring bone. The surgeon evaluates gum thickness, bite, smoking status, general health, medications, and oral hygiene. Diabetes, periodontal disease, and heavy smoking do not always rule out grafting, but they can influence healing and raise the risk of complications.
At this point, the patient should receive a clear answer to three questions: whether grafting is truly necessary, what material and method are most appropriate, and whether the implant will be placed at the same surgery or later. That clarity reduces anxiety because it turns a vague concept into a realistic medical plan.
Stage 2: preparing the site
If a failing tooth is still present, removal may be the next step. Sometimes extraction, bone preservation, and later implant placement are the safest route. In other cases, extraction is followed by immediate implant placement with simultaneous grafting. The difference depends on infection, soft tissue condition, primary stability, and anatomy.
Site preparation may also include treatment of inflammation, professional cleaning, or stabilization of gum health before surgery. This is not a formality. Bone grafting into an unhealthy environment is less predictable than grafting into a controlled, clean surgical field.
Which grafting stage comes next depends on the defect
There is no single procedure called “bone restoration.” Several protocols may be used under the same general idea of rebuilding bone before implantation.
For a narrow ridge, guided bone regeneration is often chosen. In this approach, the missing contour is rebuilt using graft material and a membrane that protects the area while new bone forms. In selected cases, additional fixation with pins or screws may be required to keep the space stable.
In the upper posterior jaw, the limiting factor is often the maxillary sinus. If bone height below the sinus is insufficient, a sinus lift may be needed. A small internal sinus lift can sometimes be done together with implant placement. A more extensive lateral sinus augmentation usually requires a separate surgical stage, especially when residual bone is minimal.
For larger defects, autogenous bone, allograft, xenograft, or a combination may be used. Each option has trade-offs. Autogenous bone has strong biological activity, but it requires a donor site. Slowly resorbing materials can help maintain volume, but healing may take longer. The best choice is the one that matches the defect size, the timeline, and the restorative plan.
Stage 3: bone augmentation surgery
The surgical stage is usually performed under local anesthesia, and in many cases the recovery is more manageable than patients expect. The procedure itself is technique-sensitive. Gentle tissue handling, tension-free closure, blood supply preservation, and stable graft fixation are what separate routine grafting from predictable grafting.
This is also where modern adjuncts can improve healing conditions. PRF, for example, may be used to support soft tissue healing and improve surgical biology. Digital planning and, when appropriate, surgical guides help align the grafting strategy with the future implant position rather than simply adding bone in a general way.
That point matters. Bone should not be rebuilt just to make the scan look better. It should be rebuilt where the implant and future crown actually need support.
Stage 4: healing and protection of the graft
After surgery, the graft needs time and stability. Depending on the technique and the amount of augmentation, healing may take from a few months to significantly longer. Small contour corrections may mature faster than vertical reconstruction or large sinus grafts.
This is the stage where patient behavior affects the result. Smoking, pressure from a removable prosthesis, poor oral hygiene, and missed follow-up visits can compromise healing. Swelling and mild discomfort are common early on, but persistent pain, unusual discharge, or wound opening require prompt review.
Follow-up appointments are not administrative add-ons. They allow the surgeon to check soft tissue closure, detect early complications, and decide whether healing is proceeding on schedule. In a well-run surgical protocol, aftercare is part of treatment, not an afterthought.
When can the implant be placed?
This is usually the most important timing question in восстановление кости перед имплантацией этапы лечения. The answer is: it depends on primary stability and the type of defect.
If enough native bone is present to stabilize the implant, grafting and implant placement may be done at the same appointment. This can shorten treatment time and reduce the number of surgeries. But it is only appropriate when stability is reliable and the defect can be predictably managed around the implant.
If native bone is insufficient, the safer route is staged treatment. First the graft heals, then the implant is placed into a more favorable foundation. This approach takes longer, but in severe atrophy it is often the more controlled and durable option.
Stage 5: reassessment after healing
Before implant placement, the site is reassessed clinically and radiographically. The surgeon confirms whether the graft has integrated, whether contour and density are adequate, and whether the soft tissue supports a stable long-term result.
Sometimes the plan remains exactly as expected. Sometimes it needs adjustment. A site may require minor additional contouring, a different implant diameter, or a revised timing protocol. This is not a setback. It is responsible surgical decision-making.
Stage 6: implant placement and restoration phase
Once the augmented area is ready, implant placement becomes more predictable because it is being done into a reconstructed, planned foundation. Depending on stability and esthetic demands, the restoration phase may begin after another healing interval.
The patient often thinks the grafting phase is separate from the implant phase, but they are closely connected. The quality of bone reconstruction influences implant position, implant stability, gum architecture, and long-term maintenance. Good grafting is not cosmetic preparation for the “real” treatment. It is part of the real treatment.
What patients should realistically expect
Bone grafting before implants is highly effective, but it is not magic and it is not identical in every clinic. Predictability depends on diagnosis, surgical technique, tissue management, patient compliance, and prosthetic planning.
The shortest plan is not always the best plan. Immediate treatment is attractive, and in the right case it is excellent. But when anatomy is unfavorable, rushing can create avoidable compromise in implant position or long-term esthetics. On the other hand, delaying everything automatically is not ideal either if simultaneous treatment can be done safely.
This is why an individualized protocol matters more than a generic timeline. In a practice focused on surgical implant dentistry, such as Implantolog.co.il, patients benefit from a plan built around anatomy and outcome rather than a one-size-fits-all sequence.
A well-executed grafting case should leave the patient with more than enough bone on a scan. It should create the conditions for an implant that is stable, cleanable, properly positioned, and comfortable for years to come. That is the standard worth aiming for, even if it takes an extra stage to get there.
Comments (0)