Losing a tooth is one problem. Losing the bone that used to support it is the part many patients do not see until implant planning begins.
This is where guided bone regeneration dental treatment becomes relevant. If the jawbone is too thin or too low in volume, placing an implant in the ideal position may be unsafe or simply impossible. In these cases, the goal is not to force the implant into compromised anatomy, but to rebuild the missing foundation first or at the same time.
For patients, that usually raises two immediate questions. Do I really need bone grafting, and how predictable is it? The honest answer is that it depends on the amount and location of bone loss, the quality of the soft tissue, sinus anatomy in the upper jaw, and the implant plan itself. When the indication is correct and the protocol is followed carefully, guided bone regeneration is a well-established method for creating the bone volume needed for long-term implant stability.
What guided bone regeneration dental treatment actually means
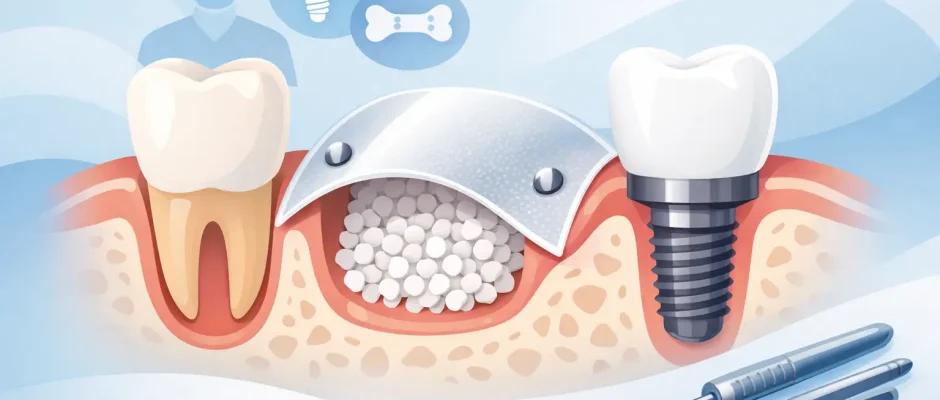
Guided bone regeneration, often shortened to GBR, is a surgical technique used to restore lost bone in the jaw. The principle is straightforward: the surgeon places bone graft material in the deficient area and then protects it with a barrier membrane. That membrane helps keep fast-growing soft tissue out of the space so slower-forming bone has the opportunity to regenerate.
The concept sounds simple, but execution matters. Bone regeneration is not just about adding graft material. It is about creating and maintaining a stable, protected space with adequate blood supply and tension-free soft tissue closure. If one of those elements is missing, the result becomes less predictable.
In implant dentistry, GBR is most often used when there is a horizontal deficiency, meaning the ridge is too narrow, or a vertical deficiency, meaning bone height is lacking. It can also be performed immediately after tooth extraction if the socket walls are damaged or if preserving ridge volume is important for future implant placement.
When GBR is recommended before or during implants
Not every implant patient needs bone regeneration. Many do not. But in everyday surgical practice, several situations make GBR a reasonable and often necessary part of treatment.
A common scenario is long-term tooth loss. After extraction, the bone begins to resorb because it is no longer loaded by the tooth root. This process is most pronounced in the first months, but it can continue over time. If too much ridge width is lost, an implant may no longer fit within the bone envelope without risking thread exposure or esthetic compromise.
Another frequent indication is infection-related bone loss. A failing tooth, root fracture, advanced periodontal destruction, or a chronic inflammatory lesion can leave behind a defect that does not provide enough support for immediate implant placement. In these cases, the timing of regeneration depends on the extent of the defect and the control of infection.
The upper posterior jaw presents a different issue. Here, bone height is often limited by the maxillary sinus. If bone is insufficient, a sinus augmentation may be required, sometimes together with GBR in the ridge area. In the esthetic zone, especially in the front upper jaw, even a moderate defect can matter because implant position and soft tissue support directly affect the visible result.
How the procedure is planned
Good GBR starts before surgery. Clinical examination and CBCT imaging are used to evaluate bone volume, defect morphology, neighboring roots, sinus anatomy, nerve position, and soft tissue conditions. This is also the stage where the surgeon decides whether the implant can be placed simultaneously or whether a staged approach is safer.
That decision is not cosmetic or arbitrary. If primary implant stability can be achieved and the defect is manageable, simultaneous implant placement with GBR may reduce treatment time and avoid an extra surgery. If the defect is larger, the soft tissue is thin, or implant stability would be compromised, staging often gives a more predictable outcome.
Digital planning improves this process because the surgeon can assess implant position prosthetically, not just anatomically. The question is not only whether an implant fits, but whether it can be placed where the future crown should be. That distinction matters.
Materials used in guided bone regeneration dental cases
Several materials may be used, and the choice depends on the defect and the treatment goals.
Bone grafting material can be autogenous, meaning taken from the patient, xenogeneic, allogeneic, or a combination. Autogenous bone has living biological potential and remains valuable in selected defects, but it requires a donor site. Particulate substitute materials are widely used because they help maintain volume and avoid additional morbidity.
The membrane can be resorbable or non-resorbable. Resorbable collagen membranes are common in routine GBR because they are easier to manage and do not require a second surgery for removal in most cases. Non-resorbable membranes may provide stronger space maintenance in certain defects, but they are technique-sensitive and carry different exposure risks.
In some protocols, biologic adjuncts such as PRF are used to support soft tissue healing and improve handling of the grafted area. These are not magic additions, but in the right hands they can contribute to a more favorable healing environment.
What the surgery feels like from the patient side
Patients often imagine bone regeneration as something more traumatic than it usually is. In most cases, the procedure is performed under local anesthesia, and the surgery itself should not be painful. What patients notice more often is pressure, vibration, and the awareness that the surgeon is working in a small, precise field.
After surgery, swelling and soreness are expected for several days. The intensity varies with the size of the graft, the surgical site, whether an implant was placed at the same time, and the patient’s biology. Upper jaw procedures and small horizontal augmentations are often easier than patients expect. Larger vertical defects or combined procedures can involve a more demanding recovery.
Postoperative discipline matters. Membrane stability and wound closure are not abstract surgical details. They depend partly on how well the patient follows instructions related to hygiene, diet, smoking cessation, medications, and follow-up visits.
Healing time and when implants can be placed
Bone regeneration is a biologic process, so healing takes time. In many staged cases, the grafted site is re-evaluated after about four to six months, though timing can vary. Dense cortical defects, vertical augmentation, sinus procedures, and patients with slower healing may require longer intervals.
This is one of the trade-offs patients should understand clearly. A faster timeline is attractive, but rushing implant placement into insufficiently matured regenerated bone can reduce predictability. The right plan is not always the shortest one.
When implants are placed simultaneously with GBR, healing still needs to respect both osseointegration and graft maturation. That is why temporary prosthetic decisions are made carefully, especially in esthetic areas or cases with larger defects.
Risks, limitations, and what affects success
Guided bone regeneration has a strong evidence base, but it is not guaranteed in every defect. Small and moderate horizontal defects are generally more predictable than large vertical reconstructions. Soft tissue thickness, defect shape, flap design, tension-free closure, patient hygiene, and smoking status all matter.
One of the more significant complications is wound dehiscence with membrane exposure. Sometimes this can be managed conservatively. In other situations, it can compromise the graft. Infection, partial graft loss, delayed healing, and insufficient final volume are also possible.
This is exactly why case selection and surgical protocol are so important. The quality of the final result depends less on the label of the material and more on diagnosis, planning, execution, and follow-up. In experienced surgical practice, the aim is not simply to add bone, but to create conditions where the future implant is stable, cleansable, and prosthetically correct.
Why experience matters in deficient bone cases
Bone loss changes the rules of implant treatment. A straightforward implant in a healed, intact ridge is one thing. An implant in a site with thin bone, previous infection, sinus proximity, or esthetic demands is another.
These are the cases where surgical judgment matters as much as technical skill. Whether to extract and graft immediately, preserve the socket, place an implant with simultaneous GBR, stage the treatment, add PRF, use a surgical guide, or combine the case with sinus lifting should be decided from imaging, anatomy, and the restorative plan, not from a one-size-fits-all template.
That is also why consultation should feel specific. A patient should leave understanding what bone is missing, why it matters, what options exist, what the timeline will be, and where the uncertainties are. Clear planning usually reduces anxiety more effectively than vague reassurance.
At implantolog.co.il, this approach is part of how complex implant surgery is structured: careful diagnostics, a precise surgical plan, and treatment chosen for predictability rather than speed alone.
If you have been told there is not enough bone for an implant, that does not automatically mean the case is hopeless or that a removable solution is your only option. It usually means the foundation needs to be rebuilt with the same level of precision expected from the implant itself.
Comments (0)