If you were told you need a sinus lift before a dental implant, the next question is usually very practical: do I need the open technique or the closed one? This is not a minor detail. The choice affects surgical access, how much bone can be added, whether implant placement can happen at the same time, and how predictable the result is in your specific anatomy.
In implant surgery, the right approach is not chosen by preference alone. It is chosen after CBCT analysis, measurement of residual bone height, evaluation of sinus anatomy, and a realistic assessment of implant stability. That is why the discussion around open vs closed sinus lift should start with diagnosis, not with labels.
What open vs closed sinus lift actually means
A sinus lift is a bone augmentation procedure in the upper back jaw. When molars or premolars have been missing for some time, the available bone under the maxillary sinus often becomes too thin for stable implant placement. The surgeon gently elevates the sinus membrane and creates space for graft material so new bone can form.
The difference between the two methods is the surgical access.
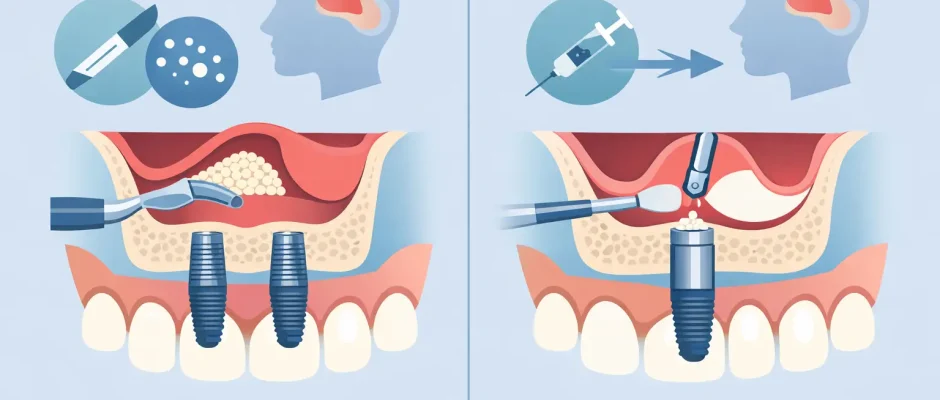
In a closed sinus lift, also called a crestal approach, the surgeon reaches the sinus floor through the implant osteotomy site. The access is from the ridge, where the implant is planned. This is a less invasive approach and is usually considered when only a modest vertical gain is needed.
In an open sinus lift, also called a lateral window approach, the sinus is accessed through a small opening in the side wall of the upper jaw. This provides much wider visibility and more control. It is generally used when the bone deficiency is more significant and a larger volume of augmentation is required.
When a closed sinus lift makes sense
A closed approach is typically chosen when there is still enough native bone to obtain primary implant stability. In practical terms, that means the remaining bone is limited, but not critically limited. The surgeon can prepare the implant site, gently elevate the sinus membrane a few millimeters, place graft material if indicated, and often place the implant in the same procedure.
For the patient, this usually means a shorter and less traumatic surgery. Swelling is often milder than with a lateral window technique, and recovery can feel easier. That said, it is not “better” in every case. It is better only when the anatomy supports it.
The limitation of the closed technique is straightforward: it does not give the same visibility or amount of vertical augmentation as an open sinus lift. If the residual bone is too thin, trying to solve the case with a crestal approach may reduce predictability. In implant surgery, a smaller procedure is not automatically a smarter procedure.
Typical indications for a closed sinus lift
The closed technique is often used when there is moderate bone loss in the posterior maxilla, the sinus floor needs only limited elevation, and simultaneous implant placement is realistic. It can be especially useful in single-tooth or short-span restorations where the anatomy is favorable and the membrane elevation required is small.
When an open sinus lift is the better option
An open sinus lift is usually recommended when the upper jaw has lost a substantial amount of vertical bone and a closed approach would not allow enough safe augmentation. By creating a lateral window, the surgeon can directly visualize the sinus membrane, elevate it over a broader area, and place a larger amount of graft material with more control.
This is often the preferred option in more advanced atrophy, in cases involving several implants in the posterior maxilla, or when the sinus anatomy is more complex. Septa inside the sinus, irregular floor shape, and significant bone deficiency can all shift the balance toward an open approach.
For some patients, the word “open” sounds alarming. Clinically, it simply means the surgeon needs better access to do the job safely and predictably. In experienced hands, this is a standard and well-established procedure.
Typical indications for an open sinus lift
The lateral window technique is commonly selected when residual bone height is too low for reliable primary stability, when greater vertical gain is required, or when multiple implant sites need augmentation in the same posterior segment. It is also useful when the surgeon expects that direct visualization will reduce the risk of technical complications.
How surgeons decide between open and closed sinus lift
The decision is based on several factors, but residual bone height is usually the key variable. If there is enough existing bone to stabilize the implant, a closed sinus lift may be possible. If there is not, an open sinus lift becomes the more predictable route.
Bone quantity is only part of the picture. Bone quality matters too. Soft, low-density posterior maxillary bone may look acceptable on a measurement and still provide weaker implant stability than expected. Sinus anatomy also matters. A thick membrane, a very thin membrane, sinus septa, previous inflammation, or localized pathology can all change the surgical plan.
The treatment sequence is another factor. Sometimes the implant and sinus lift can be performed at the same visit. In other cases, especially with severe atrophy, it is safer to graft first, allow healing, and place the implant later. That is not a delay for the sake of delay. It is a way to protect the final result.
Healing, discomfort, and recovery
Patients often expect the closed technique to mean almost no recovery and the open technique to mean a difficult one. Reality is usually more balanced.
A closed sinus lift is generally associated with less postoperative swelling and less surgical trauma. Many patients return to normal routine quickly, with standard precautions such as avoiding nose blowing, sneezing with the mouth closed, heavy pressure changes, and intense physical strain during early healing.
An open sinus lift usually causes more swelling and requires more patience in the first postoperative days. Still, with careful microsurgical technique, proper suturing, clear instructions, and close follow-up, recovery is usually manageable. The first week is the most noticeable. Bone maturation, however, takes much longer than soft tissue healing, which is why implant timing must be planned with discipline.
Adjuncts such as PRF and precise graft handling may support healing quality, but they do not replace proper case selection. The best recovery starts with the right diagnosis.
Risks and trade-offs
Both techniques are predictable when properly indicated, but neither is risk-free. The main intraoperative concern is perforation of the sinus membrane. Small perforations can often be managed during surgery. Larger ones may require a change in plan.
In a closed sinus lift, visibility is limited, so membrane elevation is more controlled by tactile feedback. In an open sinus lift, visibility is better, but the procedure is more extensive. That is the central trade-off in open vs closed sinus lift: less invasiveness versus greater access and control.
Other possible issues include bleeding, graft migration, sinusitis, delayed healing, or insufficient bone formation. Smoking, uncontrolled periodontal disease, poor oral hygiene, and untreated sinus problems can increase complication risk. This is one reason why comprehensive surgical planning matters more than the name of the technique.
Does one method last longer or work better?
Patients understandably want a simple answer, but long-term success depends far more on indication, execution, implant position, prosthetic planning, and maintenance than on whether the sinus lift was open or closed.
If a closed sinus lift is used in a case that truly qualifies for it, outcomes can be excellent. If severe atrophy is forced into a closed approach because it seems easier, predictability drops. The same logic applies in reverse. An open sinus lift is not excessive if the anatomy requires it. It is appropriate treatment.
This is where digital planning and surgical discipline make a real difference. CBCT-based assessment, accurate implant positioning, and careful respect for biological limits are what turn augmentation into a stable foundation rather than a temporary fix. On https://implantolog.co.il, this philosophy is central: choose the least traumatic approach that still gives a safe and predictable result.
Questions worth asking at your consultation
If you are comparing options, ask how much native bone is present, whether the implant can be placed at the same time, how much vertical gain is needed, and what makes one approach more predictable in your case. Ask about sinus anatomy, healing time, and what the backup plan is if membrane perforation occurs. These are practical questions, and a surgeon who works with sinus augmentation regularly should answer them clearly.
The right plan should feel medically justified, not improvised. When patients understand why a specific technique was chosen, anxiety usually drops. Clarity is part of surgical care.
A sinus lift is not a goal by itself. It is a preparatory step that creates the conditions for a stable implant in an area where bone is often limited. The best choice between open and closed is the one that respects your anatomy, your restorative plan, and the need for a durable result years after the surgery is forgotten.
Comments (0)