If you were told you need a sinus lift before an implant, the real question is usually not whether the procedure exists. It is which approach fits your anatomy: open or closed.
That distinction matters because these are not interchangeable techniques. They solve the same problem – limited bone height in the upper back jaw – but they do it differently, with different indications, surgical access, healing timelines, and expectations. For patients, the best choice is rarely about choosing the “easier” option. It is about choosing the method that gives the implant the highest chance of long-term stability.
Open vs closed sinus lift – what is the difference?
A sinus lift is a bone augmentation procedure used in the posterior maxilla, usually in the premolar and molar region, when the floor of the maxillary sinus sits too low for predictable implant placement. After tooth loss, bone in this area often resorbs, while the sinus may expand downward. The result is simple: there is not enough vertical bone for an implant of proper length and stability.
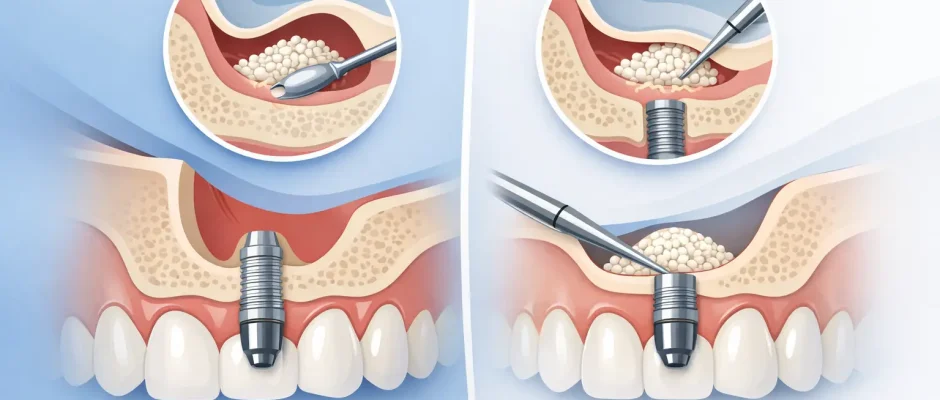
In an open sinus lift, the surgeon creates access through the lateral wall of the sinus. The sinus membrane is carefully elevated, and graft material is placed beneath it to increase bone volume. This approach gives direct visibility and greater control, which is why it is often chosen in more pronounced bone deficiency.
In a closed sinus lift, also called a crestal approach, access is created through the implant osteotomy from the top of the ridge. The membrane is elevated indirectly, and a smaller amount of graft may be added. This is a less invasive option, but it is suitable only when there is already enough native bone to support primary implant stability.
The difference, then, is not only surgical access. It is how much vertical gain is needed, how much native bone remains, and whether an implant can be stabilized at the same stage.
When an open sinus lift is usually the better choice
An open approach is generally considered when residual bone height is limited, often in the range where implant stability cannot be predictably achieved with a crestal technique alone. Exact thresholds vary by case, CBCT findings, implant design, and the quality of the remaining bone, but severe vertical deficiency typically points toward an open sinus lift.
This method is more technique-sensitive, yet it is also more versatile. It allows broader membrane elevation, better management of sinus anatomy, and more substantial bone augmentation. If the sinus floor is highly pneumatized, if multiple adjacent implants are planned, or if the case involves complex reconstruction, the open approach often provides the safest and most predictable route.
That does not automatically mean implants must always be delayed. In some cases, implants can be placed simultaneously if primary stability is achievable. In others, grafting is performed first and implant placement is staged after healing. The decision depends on residual bone, torque expectations, and the overall restorative plan.
When a closed sinus lift makes sense
A closed sinus lift is typically chosen when the bone deficiency is mild to moderate and there is enough native bone to stabilize the implant at the time of surgery. This is the main advantage of the crestal approach: treatment may be less invasive while still solving the problem.
For the patient, closed sinus lift often means a smaller surgical field, less postoperative swelling, and a somewhat easier recovery. But those benefits apply only when the indication is correct. Trying to use a closed approach in a case that really requires an open one can compromise both graft maturation and implant stability.
This is why proper planning matters more than the label of the technique. A minimally invasive procedure is valuable only when it remains biologically sound.
Open vs closed sinus lift – which one heals faster?
In straightforward cases, a closed sinus lift is usually associated with a lighter postoperative course. Patients may experience less swelling and discomfort because tissue elevation and surgical access are more limited.
An open sinus lift can involve more swelling, occasional bruising, and a longer period of awareness in the surgical area. That said, healing is not judged only by how you feel in the first few days. Biological healing and readiness for loading depend on graft integration, implant stability, membrane integrity, and the amount of augmentation performed.
So the practical answer is nuanced. Closed sinus lift often feels easier early on. Open sinus lift may require more recovery upfront, but in advanced bone loss it can be the more predictable path to a durable result. In implant surgery, predictability is more important than short-term convenience.
What determines the right choice
The most important factor is not preference but diagnosis. A CBCT scan shows the vertical bone height, ridge width, sinus anatomy, septa, membrane condition, and other details that directly affect treatment planning.
Several clinical variables guide the choice between open and closed sinus lift. Residual bone height is central, but not the only issue. Bone density, sinus width, the presence of septa, previous inflammation, smoking, periodontal history, and whether a single implant or a multi-unit restoration is planned all influence the protocol.
The surgeon also has to think beyond augmentation alone. The real endpoint is not “bone added.” The endpoint is a stable, correctly positioned implant that supports a functional and esthetic restoration over time. A technique should be selected because it serves that endpoint, not because it sounds simpler.
Does one method have more risks?
Both procedures are well established, but neither is risk-free. The most discussed intraoperative complication is sinus membrane perforation. Small perforations can often be managed successfully during surgery, but risk increases with difficult anatomy, thin membranes, or limited visibility.
Because an open sinus lift gives direct access to the lateral wall and membrane, it may offer better control in advanced cases. A closed sinus lift is less invasive, but visibility is more limited, so case selection becomes especially important.
Other possible issues include infection, graft loss, sinus symptoms, delayed healing, or insufficient bone formation. These are not routine outcomes, but they are part of informed consent. Good planning, careful microsurgical technique, and appropriate postoperative instructions reduce risk significantly.
This is one reason experienced surgical judgment matters so much in sinus augmentation. The procedure is not only about placing graft material. It is about respecting anatomy and controlling variables that affect healing.
What patients usually want to know before surgery
Most patients ask three practical questions: Will it hurt, will the implant be placed the same day, and how long until the final tooth?
With modern local anesthesia and careful technique, the procedure itself is typically well tolerated. What patients describe afterward is usually pressure, swelling, and mild to moderate soreness rather than sharp pain. Recovery varies, especially between open and closed approaches, but most people can return to normal routine quickly with a few temporary restrictions.
Whether the implant is placed at the same time depends mainly on primary stability. If there is enough native bone to stabilize the implant, simultaneous placement may be possible. If not, staging is safer. This is not a setback – it is often the more responsible path when anatomy demands it.
As for timing, final restoration is dictated by healing biology, not by calendar pressure. Rushing an implant in a grafted posterior maxilla is rarely a smart trade.
Why technique alone does not guarantee a good result
A sinus lift is never just open or closed. The outcome also depends on imaging, implant planning, graft strategy, membrane handling, soft tissue management, and postoperative follow-up.
In a modern surgical workflow, digital diagnostics improve precision before the first incision. In selected cases, guided implant planning, atraumatic protocols, and biologically supportive measures such as PRF can help support healing and reduce variability. None of these replace surgical skill, but together they make treatment more controlled and more transparent for the patient.
That is the standard many patients are looking for when they compare options for implant treatment in complex upper-jaw cases. If you are evaluating sinus augmentation in Israel, including treatment planning in Tel Aviv, the value is not just in having the procedure available. It is in having a clear rationale for why one approach is being recommended over the other.
The better question to ask at consultation
Instead of asking, “Which sinus lift is better?” ask, “Which option gives me the most predictable implant stability in my anatomy?”
That question changes the discussion. It moves attention away from marketing terms and toward diagnosis, safety, and long-term function. A closed sinus lift can be excellent when the indication is right. An open sinus lift can be the more conservative choice when bone is severely limited. Conservative does not always mean smaller surgery. Sometimes it means choosing the method with the best margin of safety.
A good treatment plan should make that logic easy to understand. You should know how much bone is available, whether implant placement is immediate or staged, what the recovery is likely to feel like, and what milestones matter before the final restoration.
When the plan is built around anatomy rather than guesswork, the procedure becomes less intimidating – and the result becomes far more predictable.
Comments (0)