When a tooth has to be removed, most patients ask the same practical question: can it be replaced right away, or will there be months without a tooth? In many cases, имплантация после удаления с немедленной нагрузкой is a real option. But it is not a universal shortcut. The result depends on anatomy, infection control, bite forces, soft tissue condition, and the precision of the surgical plan.
For the right patient, this protocol can reduce the number of surgeries, preserve gum contours more predictably, and shorten the path from extraction to a fixed tooth. For the wrong case, rushing can increase the risk of implant instability, recession, or esthetic compromise. That is why the decision is made not by calendar alone, but by clinical criteria.
What immediate implant placement with immediate loading actually means
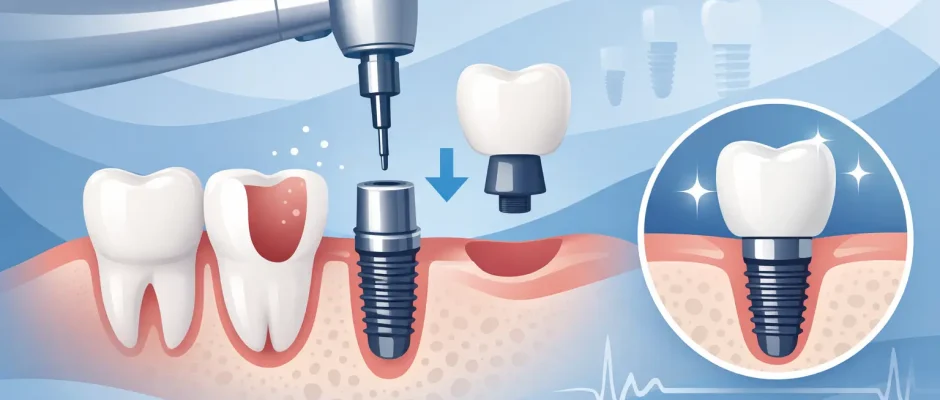
These terms are often used loosely, and that creates confusion. Immediate implant placement means the implant is inserted into the extraction site during the same appointment as the tooth removal. Immediate loading means a temporary crown or restoration is connected very soon after surgery, often the same day or within a few days.
Those are two separate decisions. A surgeon may place the implant immediately but leave it unloaded under the gum to protect healing. In other cases, the implant can be placed and restored with a temporary tooth right away. The second scenario sounds more attractive, but it requires stricter conditions.
The key issue is primary stability. The implant must engage bone firmly enough at surgery to tolerate a provisional restoration without harmful micromovement during healing. This is one reason why digital planning, CBCT imaging, and in selected cases surgical guides matter – they improve control over implant position, angulation, and the use of available native bone beyond the socket.
When имплантация после удаления с немедленной нагрузкой is a good option
The best candidates are patients with enough residual bone to stabilize the implant, healthy or controllable soft tissue, and no uncontrolled acute infection that compromises the site. The bite also matters. A front tooth that can be kept out of heavy contact is very different from a molar under strong chewing load or a patient with bruxism.
A favorable case often includes an atraumatic extraction, preserved socket walls, especially the facial bone, and the ability to place the implant in a prosthetically correct position. If the temporary crown can be designed mainly for appearance rather than function during early healing, the prognosis improves.
This is especially useful in the esthetic zone. When a visible tooth is removed, preserving the natural architecture of the gum is often just as important as integrating the implant. Immediate placement and carefully managed temporization can help support the soft tissue profile. Even then, “can be done” is not the same as “should be done.” In a thin gum phenotype or when the facial plate is damaged, staged treatment may be safer and more predictable.
When it is better to slow down
Not every extraction site should receive an implant immediately, and not every immediate implant should be loaded right away. Severe bone loss, uncontrolled periodontal inflammation, active suppuration, lack of apical or palatal bone for fixation, or high occlusal load may all shift the plan toward a delayed approach.
Sometimes the most responsible decision is to preserve the socket first, allow soft and hard tissues to heal, and place the implant later under better conditions. This is not a failure of planning. It is often the better biology.
A common example is a tooth with a large chronic infection and destruction of surrounding bone. In some of these cases, immediate placement is still possible after thorough debridement. In others, the risk-benefit balance is not favorable. The choice depends on the exact defect morphology, tissue quality, and ability to obtain stable fixation away from the compromised socket walls.
How the procedure is planned
Good results start before the extraction. Clinical examination and 3D imaging are used to assess root anatomy, bone volume, proximity to vital structures, and the future restorative position of the tooth. The implant is not placed where the old root happened to be. It is placed where the final tooth needs proper support.
This is why prosthetically driven planning is essential. The surgeon evaluates whether the implant can be anchored beyond the extraction socket, whether simultaneous bone grafting is required, and whether a temporary crown can be placed without functional loading. In selected cases, guided surgery helps translate that plan with higher precision.
Micro-surgical technique also matters. The less trauma to the socket walls and soft tissue, the better the chance of preserving contours. Adjuncts such as PRF may support soft tissue healing and help manage the surgical site, but they do not replace sound indications or careful execution.
What happens on the day of treatment
The sequence is usually straightforward but technically demanding. The tooth is removed as atraumatically as possible. The socket is cleaned carefully to remove granulation tissue or inflammatory remnants. The implant osteotomy is then prepared in native bone, often beyond or around the socket rather than simply within it.
If sufficient primary stability is achieved, a temporary restoration may be delivered. In many anterior cases, that temporary crown is intentionally kept out of direct biting contact. It looks like a tooth, but it is not meant for normal chewing during early healing.
If there is a gap between the implant and the socket wall, bone graft material may be used to support contour preservation. Depending on the situation, the surgeon may also use connective tissue grafting or contour management to improve soft tissue stability and esthetics.
Risks and trade-offs patients should understand
The appeal of finishing more in one stage is obvious, but the biology does not become simpler just because the timeline is shorter. Immediate protocols are technique-sensitive. The implant can integrate well and still end up with gum recession or a compromised emergence profile if tissue management is not ideal.
There is also a difference between survival and success. An implant that remains in the mouth is not automatically a great result if the gums collapse, the temporary crown overloads the fixture, or the final esthetics are poor. In the back of the mouth, immediate loading may be less forgiving because chewing forces are higher. In patients who clench or grind, protection and case selection become even more important.
This is why experienced surgeons are careful with promises. Same-day teeth are possible, but not every same-day solution is equal in function, esthetics, or long-term predictability.
Healing and the final crown
Even when a temporary tooth is placed immediately, healing still takes time. Osseointegration usually develops over weeks to months depending on bone quality, implant stability, and the clinical scenario. During this period, follow-up visits are important. The temporary restoration may need adjustment to protect the implant and shape the surrounding soft tissue.
The final crown is placed only when the implant is stable and the tissue architecture is ready. Rushing this stage can compromise the result. A well-shaped provisional often acts as a blueprint for the final restoration, especially in the smile zone where tiny contour changes affect appearance.
Patients sometimes assume that immediate loading means the treatment is finished in one day. It is more accurate to say that the visible gap can often be addressed immediately, while the biologic integration still follows its own timeline.
Why surgeon experience changes the outcome
This protocol rewards precision. It demands control of extraction technique, implant positioning, soft tissue management, grafting decisions, and restorative planning. It also requires judgment – knowing when to proceed and when not to.
That judgment is particularly important in complex cases: thin facial bone, previous endodontic infection, failed crowns, root fractures, or esthetically demanding front teeth. Digital planning and surgical guides improve accuracy, but technology does not replace surgical discipline. The best outcomes usually come from combining both.
For patients seeking treatment in Israel, especially in clinically demanding cases, it makes sense to choose a surgeon who regularly works with immediate protocols, bone augmentation, and microsurgical soft tissue techniques. That combination often determines whether the result is merely fast or genuinely predictable. You can learn more about this approach at https://implantolog.co.il.
The right question to ask at consultation
Instead of asking, “Can I get an implant the same day?” ask, “Am I a good candidate for a stable and esthetic result with this protocol?” That shifts the conversation toward what actually matters: bone support, infection control, tissue quality, bite forces, and long-term planning.
In many cases, имплантация после удаления с немедленной нагрузкой is an excellent solution. In others, a staged approach is the safer path to the better result. The goal is not to move fast at any cost. The goal is to remove uncertainty, protect the tissues you have, and build a restoration that feels dependable from the first day to the final crown.
Comments (0)