A root canal that was done years ago can stay quiet for a long time – until a scan shows persistent inflammation near the tip of the root, or the tooth starts aching when you bite. In that situation, the question behind the search query “when is an apicoectomy really necessary” is very practical: can the tooth still be saved, and is surgery really the right next step?
Apicoectomy, or root-end resection, is a tooth-preserving microsurgical procedure. The goal is not simply to “cut something off,” but to remove the infected tissue around the root tip, resect the very end of the root, seal it properly, and stop the source of chronic inflammation. When done for the right indication, it can allow a natural tooth to remain functional for years.
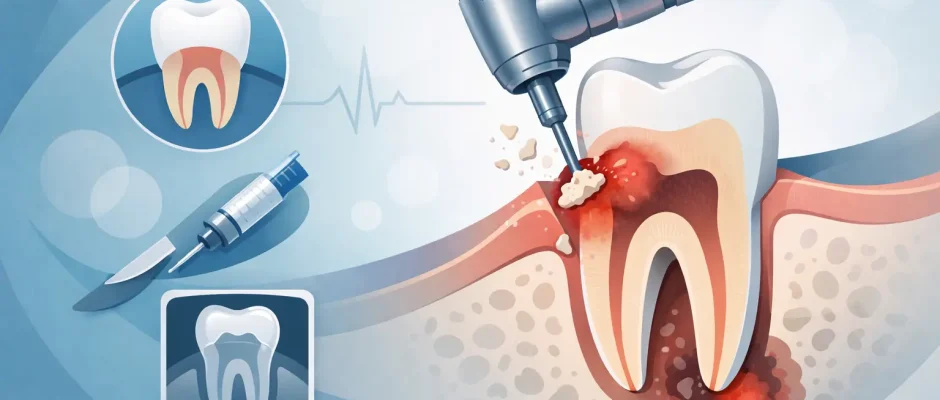
Apicoectomy: When Is Root-End Surgery Really Necessary?
This operation is usually considered after endodontic treatment has failed or when nonsurgical retreatment is unlikely to solve the problem predictably. The key point is that apicoectomy is not the first-line treatment for every tooth with a dark spot on an X-ray. In many cases, retreating the root canal from inside the tooth is preferable. In others, surgery offers a cleaner and more controlled solution.
A root-end surgery becomes relevant when there is persistent apical periodontitis – inflammation or a cyst-like lesion near the root tip – despite previous root canal treatment. It is also indicated when a post, crown, or complex restoration makes conventional retreatment risky or destructive. Removing an expensive, well-fitting crown just to access the canals may weaken the tooth, and sometimes the anatomy or obstruction inside the canal makes retreatment incomplete.
Another common indication is the presence of a fractured instrument, ledge, calcification, or other blockage in the canal that prevents proper cleaning of the apical part of the root. In that setting, approaching the root from the outside may be more predictable than trying to force access through a difficult canal.
Surgery may also be recommended when there is an anatomical problem near the root tip, such as apical resorption, overfilling with symptomatic material beyond the apex, or a persistent lesion that has not healed after adequate waiting time. If the tooth is strategically important – for example, supporting your bite or part of a larger restorative plan – preserving it can have real functional value.
When surgery is useful and when it is not
Not every infected tooth is a good candidate for root-end resection. The success of the procedure depends on diagnosis, root anatomy, periodontal support, crack status, and restoration quality. That is why a 3D scan is often more valuable than a standard X-ray alone.
An apicoectomy can make sense if the tooth has enough healthy structure above the gumline, stable surrounding bone support, and no vertical root fracture. It is especially useful for front teeth and premolars, where surgical access is often more straightforward. Molars can also be treated, but the decision is more selective because access is harder and anatomy is more complex.
On the other hand, surgery is usually not the best option if the tooth has a vertical root fracture, severe mobility, advanced periodontal destruction, or decay extending too far below the gumline. In those cases, removing the source of infection by extraction may be the safer and more predictable choice. The same applies when the tooth cannot be restored properly even if the inflammation is removed.
This is one of the most important trade-offs patients should understand: saving a tooth is valuable, but only if the tooth has a realistic long-term prognosis. Surgery should not be used to delay an inevitable extraction if the structural foundation is already lost.
How the decision is made
The question “when is an apicoectomy really necessary” cannot be answered by symptoms alone. Some teeth with significant inflammation cause no pain at all. Others hurt because of a bite issue, crack, or gum inflammation rather than a lesion at the root tip.
A proper decision usually starts with a clinical exam, vitality and percussion findings where relevant, periodontal evaluation, and imaging. Cone beam CT is often the deciding tool because it shows the true size and position of the lesion, the relation to nearby anatomical structures, missed canals, root shape, and possible perforations or fractures.
The clinician also evaluates whether retreatment through the crown is realistic. If the old root canal filling is clearly short, incomplete, or poor in quality, and access is feasible without major destruction, nonsurgical retreatment may come first. If access is blocked or the tooth already has a stable restoration that would be costly or risky to remove, microsurgery may be the more conservative path overall.
This is where an experienced surgical approach matters. Modern apicoectomy is not the same as older, more aggressive surgery. Under magnification, with microsurgical instruments and root-end filling materials designed for biocompatibility, treatment becomes more precise and tissue trauma is reduced.
What happens during an apicoectomy
The procedure is typically performed under local anesthesia. A small flap is raised, the infected tissue around the root tip is removed, and the last few millimeters of the root apex are resected. The root end is then prepared and sealed from the surgical side to reduce the chance of bacterial leakage.
In selected cases, regenerative support may be added, especially if there is a significant bone defect. Depending on the anatomy and defect configuration, this can improve healing conditions. The exact protocol depends on the tooth and the lesion, not every case needs added grafting materials.
From the patient perspective, the surgery is usually less dramatic than the name sounds. With careful soft-tissue handling and modern microsurgical technique, postoperative discomfort is often manageable and short-lived. Swelling can occur, but many patients compare recovery to a routine extraction rather than a major operation.
Recovery and healing expectations
Most people can return to normal non-strenuous activity within a day or two. Mild soreness, swelling, and tenderness are expected early on. The bone, however, heals much more slowly than the soft tissue. Even when you feel fine after a week, radiographic healing can take months.
Follow-up matters because the success of the surgery is judged not only by symptom relief but also by reduction or resolution of the lesion over time. A tooth may feel comfortable long before the bone looks fully healed on imaging.
It is also worth knowing that perfect healing is not guaranteed in every case. Success rates are generally good when diagnosis, case selection, and surgical technique are strong, but they are lower if there is an undetected crack, missed canal anatomy, or poor coronal seal. That is why the quality of the existing restoration still matters after surgery.
Apicoectomy vs extraction and implant
Patients often ask a direct question: why not just remove the tooth and place an implant? Sometimes that is the right answer. But not always.
A well-treated natural tooth is still a very valuable structure. If the tooth can be predictably preserved, keeping it may reduce treatment complexity, shorten rehabilitation, and avoid additional procedures such as extraction site preservation or bone augmentation. Preserving your own tooth also maintains natural proprioception, which implants do not replicate.
At the same time, extraction and implant placement may be the better plan if the tooth has multiple risk factors – fracture, poor ferrule, recurrent deep decay, failed prior surgery, or severe bone loss. In those situations, repeated attempts to save the tooth can increase cost, treatment time, and frustration without improving the final prognosis.
The right choice is not ideological. It is clinical. The best plan is the one with the most predictable long-term result, not the one that sounds more conservative or more high-tech.
Signs you may need evaluation sooner
Persistent tenderness when chewing, a gum bump that drains near the tooth, recurring swelling, or discomfort around a previously treated root canal are good reasons to get the area checked. The same applies if imaging done for another reason shows a lesion near the root tip, even if the tooth is not hurting.
Some chronic infections remain surprisingly silent. Waiting for severe pain is not a reliable strategy. Earlier evaluation often means more options and a more controlled treatment plan.
In a surgical practice focused on tooth preservation, implantology, and microsurgical protocols, the value is not just performing the procedure – it is choosing it only when it truly improves prognosis. That is the point of careful diagnostics and a clear treatment sequence.
If you have been told that a root canal tooth still shows infection, the useful next question is not whether surgery sounds scary. It is whether the tooth is structurally worth saving and which approach gives it the best chance to heal well and stay functional.
Comments (0)