Bone Loss in Jaw: Causes and Treatment
A patient often learns about jawbone loss only when planning an implant and hearing, “There may not be enough bone.” By that point, the process has usually been developing quietly for months or years. Bone loss in jaw – causes and treatment – is not just a technical issue on a scan. It affects stability, facial support, chewing function, and the predictability of future dental work.
The good news is that bone loss in the jaw can often be slowed, managed, and in many cases rebuilt enough for functional and esthetic rehabilitation. The right treatment depends on why the bone was lost, how much volume remains, and what final result is planned – saving a tooth, preparing for an implant, or restoring a full arch.
What causes bone loss in jaw?
Jawbone is living tissue. It remodels constantly in response to pressure, inflammation, infection, and blood supply. When normal stimulation disappears or chronic disease is present, the bone begins to resorb. This is why the cause matters so much: two patients may have similar scans but require very different treatment strategies.
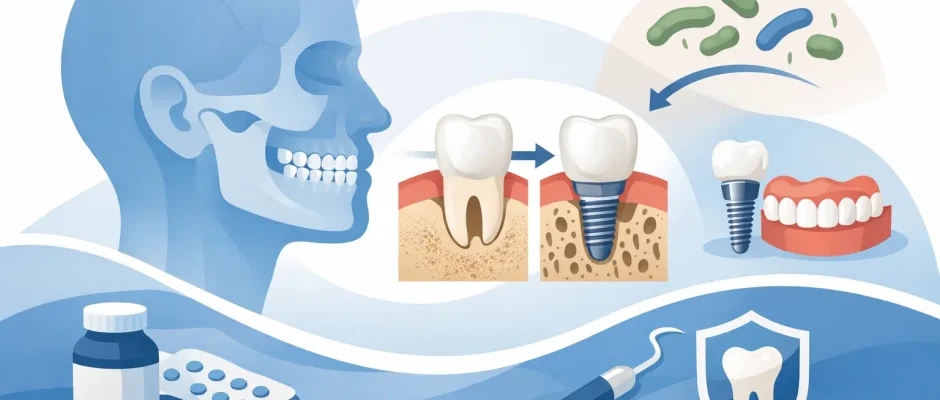
The most common reason is tooth loss. After an extraction, the bone that used to support the tooth no longer receives the same functional load. The body starts reducing that unused volume, especially during the first months after removal. This shrinkage is normal to a degree, but in some areas it becomes significant enough to complicate implant placement or affect gum contours.
Periodontal disease is another major cause. In this situation, bacteria and the body’s inflammatory response gradually destroy the supporting tissues around the teeth, including bone. Patients do not always feel pain, which is why advanced bone loss may exist even when daily function seems acceptable. Mobility, bleeding gums, bad breath, and changes in tooth position are common warning signs.
Long-standing infection at the root of a tooth can also damage surrounding bone. A chronic abscess, cystic lesion, or untreated failed root canal may create a localized defect. Sometimes the bone can recover after proper treatment. Sometimes regenerative surgery is needed.
Trauma, pressure from impacted teeth, ill-fitting dentures, smoking, uncontrolled diabetes, and certain systemic conditions can worsen the picture. In the posterior upper jaw, anatomy adds another factor: after tooth loss, the maxillary sinus may expand downward, reducing the available bone height for implants.
How jawbone loss is diagnosed
Clinical examination gives part of the answer, but treatment planning should not rely on guesswork. Bone width, height, soft tissue quality, bite, infection status, and neighboring anatomy all matter. Standard dental X-rays are useful, yet they do not always show the full three-dimensional defect.
For many surgical cases, a CBCT scan is the key diagnostic tool. It allows the surgeon to evaluate how much bone is actually present, where important structures are located, and whether implant placement is possible immediately or only after augmentation. This step is especially important in complex cases, where a seemingly minor deficiency on a regular X-ray may turn out to be a major limitation in three dimensions.
Diagnosis is not just about measuring millimeters. It is also about understanding timing. Active periodontal disease must be stabilized. Residual infection must be controlled. If a tooth can be saved predictably, that may be preferable to extraction. If not, the extraction plan should include preservation of bone from the start.
Why early treatment changes the whole plan
One of the most costly mistakes in implant dentistry is waiting too long after a tooth becomes non-restorable. The longer an area remains without functional stimulation, the more bone and soft tissue can disappear. That does not mean every missing tooth requires urgent surgery, but it does mean early evaluation creates more options.
For example, immediate implant placement after extraction may help reduce post-extraction collapse in selected cases. It is not suitable for every patient and not every socket, especially where infection, thin bone walls, or poor soft tissue conditions are present. But when indications are correct and the protocol is carefully followed, it can shorten treatment and preserve anatomy better than delayed treatment.
If immediate placement is not advisable, ridge preservation at the time of extraction can make a major difference. This approach typically uses grafting material and, when indicated, a membrane to limit shrinkage of the socket. It does not stop all remodeling, but it can preserve enough structure to simplify later implant placement.
Bone loss in jaw – causes and treatment options
Treatment is never one-size-fits-all. The goal may be to stop further loss, regenerate a defect around an existing tooth, rebuild bone for an implant, or create support for a full-arch restoration. The technique is chosen based on the defect type, not just the desire to place an implant quickly.
When periodontal disease is the driver, the first step is controlling inflammation. Without that, grafting is unstable and long-term results are compromised. Periodontal therapy may include deep cleaning, surgical access, and in selected defects, regenerative procedures that aim to restore lost supporting tissues.
When the issue follows extraction or long-term missing teeth, bone grafting is often part of treatment. Guided bone regeneration is commonly used for localized ridge deficiencies. In simple terms, bone graft material is placed where volume is missing, and the area is protected with a membrane so the body can form new hard tissue more predictably. The exact materials and technique vary according to the size and shape of the defect.
In the upper back jaw, sinus lift surgery may be needed if sinus expansion has reduced the available height. This can be done through different approaches depending on how much native bone remains. In some cases, implants can be placed at the same time. In others, staged treatment is safer.
For severe atrophy, especially in patients missing many teeth for years, the plan can become more complex. Options may include block grafting, staged augmentation, or strategic implant planning for full-arch solutions such as All-on-4. Here, the trade-off is important: some patients benefit from extensive reconstruction to optimize ideal implant positions, while others are better served by a prosthetically driven solution that avoids unnecessary grafting.
Can bone grow back on its own?
This depends on the cause and the severity. Mild bone remodeling after extraction is natural, but significant lost ridge volume usually does not fully regenerate on its own. Bone around teeth affected by periodontal disease may show some improvement once inflammation is eliminated, yet advanced structural loss rarely reverses without targeted treatment.
The body can heal, but it heals according to biology, not according to prosthetic plans. If the future goal is an implant in an ideal position, relying on spontaneous recovery is often not enough.
What affects the success of treatment
Technique matters, but so does case selection. Stable gums, good oral hygiene, controlled medical conditions, and smoking reduction all improve healing. The surgeon’s planning is equally important. Digital diagnostics, prosthetically guided positioning, and in appropriate cases surgical guides can reduce error and increase predictability.
Modern protocols may also include biologic support such as PRF, which uses the patient’s own blood-derived growth factors to support healing. It is not magic and it does not replace sound surgical principles, but in the right setting it can improve soft tissue response and postoperative comfort.
Patients often ask whether grafting is painful. In most cases, discomfort is manageable and usually less severe than expected, especially when surgery is carefully performed and postoperative instructions are clear. What creates more problems is not the graft itself, but underestimating healing time. Bone regeneration is slow tissue healing. Rushing to the next stage can jeopardize the result.
When should you seek evaluation?
If you have a missing tooth, loose teeth, chronic gum bleeding, recurrent swelling, a denture that has become unstable, or you were told you are “not a candidate” for implants because of limited bone, that is the right time for a proper surgical assessment. “Not enough bone” is often the beginning of planning, not the end of it.
In a referral-based and complex implant practice, these are common scenarios rather than exceptions. With accurate imaging and a clear sequence of treatment, many patients who assume they have run out of options can still be restored safely and predictably.
The most useful next step is not to search for the fastest fix, but to understand the biology of your specific case. Once the cause of bone loss is clear, treatment becomes far more precise – and much less intimidating.
Comments (0)