Bone Graft Before Implant Placement
When a patient is told they need a bone graft before implant placement, the usual reaction is not excitement – it is frustration. Many people come in expecting a missing tooth to be replaced with an implant right away, and hearing that an additional surgical step is necessary can feel like a delay. In reality, grafting is often the step that makes the final result safer, more stable, and more esthetic.
Dental implants depend on bone volume and bone quality. An implant is not simply inserted into the gum where the tooth used to be. It needs a three-dimensional foundation of healthy bone that can hold it firmly during healing and support the tissues around it for years. If that foundation is too thin or too low, placing an implant immediately may increase the risk of poor positioning, soft tissue recession, or failure of integration.
Why bone graft before implant placement is sometimes necessary
Bone loss begins quickly after a tooth is removed. The jaw no longer receives the same functional stimulation through the tooth root, and the ridge starts to shrink. In some patients this loss is modest. In others, especially after infection, trauma, long-term missing teeth, or periodontal disease, the change is significant.
The key issue is not only whether there is enough bone to physically fit an implant. The more important question is whether the implant can be placed in the correct prosthetic position and surrounded by enough bone to remain stable over time. An implant that is forced into compromised anatomy may survive, but survival alone is not the standard. The goal is a predictable, durable, comfortable result that also looks natural.
This is why grafting is often recommended before implant therapy in the front teeth, where esthetics matter greatly, and in posterior areas where the sinus or nerve limits the available bone height. In both situations, the surgeon is working not just to place titanium in bone, but to create the conditions for long-term function.
What a bone graft is actually trying to achieve
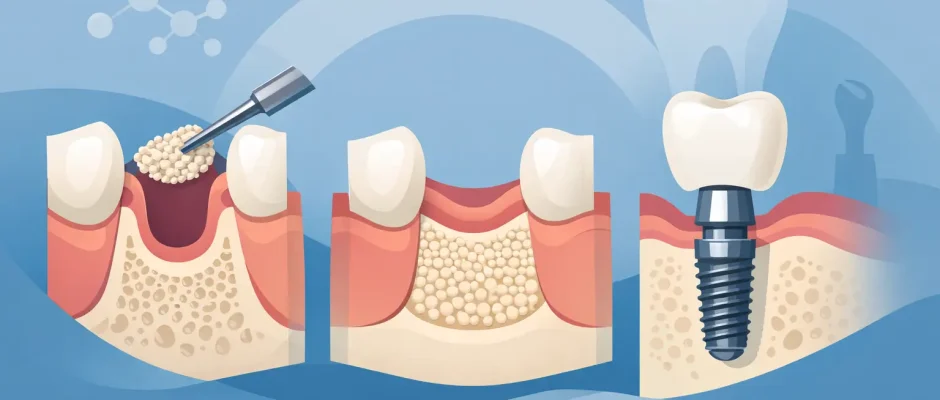
A bone graft is not a filler placed for cosmetic reasons. It is a biologic scaffold or regenerative material used to rebuild lost volume and support new bone formation. Depending on the clinical situation, the goal may be to widen a thin ridge, increase vertical height, preserve the socket after extraction, or prepare the area for a sinus lift.
There is no single grafting approach that fits every patient. Sometimes a small socket preservation procedure after extraction is enough. In other cases, guided bone regeneration with particulate graft and a membrane is needed. More advanced defects may require block grafting or staged reconstruction. The decision depends on the defect geometry, soft tissue condition, infection history, loading demands, and esthetic requirements.
In modern surgical practice, planning is increasingly digital. A CBCT scan allows precise evaluation of bone dimensions and nearby anatomy. This matters because grafting should be done with the final implant position in mind. In complex cases, the future crown, implant axis, and available bone are planned together rather than as separate steps.
Can the graft and implant be done at the same time?
Sometimes yes, and sometimes no. This is one of the most common points of confusion.
If the defect is limited and primary implant stability can still be achieved, simultaneous implant placement with grafting may be possible. This is often done when the ridge has a small dehiscence or when an implant is placed immediately after extraction with a minor gap around it. In these cases, the implant gains enough mechanical stability from the native bone, while the graft helps rebuild the contour around it.
If the site is too deficient, placing the implant at the same surgery may not be safe. When there is not enough bone to stabilize the implant properly, a staged approach is usually better. The graft is placed first, allowed to heal and mature, and the implant is inserted later into a more favorable site.
This is not over-treatment. It is often the more conservative and biologically sound choice.
How long do you wait after a bone graft before implant placement?
Healing time depends on the size of the graft, the material used, blood supply, soft tissue closure, and the patient’s biology. A small socket graft may be ready for implant placement in a few months. Larger guided bone regeneration procedures or sinus augmentation may require a longer interval.
The answer is rarely based on the calendar alone. The site needs to be clinically stable and radiographically mature enough to support implant placement with good primary stability. In some situations, healing progresses quickly. In smokers, patients with uncontrolled diabetes, or sites with previous infection and scarred tissue, the timeline may be slower.
This is where careful follow-up matters. The decision to move forward should be based on examination and imaging, not on optimism.
Materials used for grafting
Patients often ask whether the graft is their own bone or a substitute material. Both are used in implant dentistry, and each has strengths.
Autogenous bone, taken from the patient, has strong biologic potential but requires a donor site and adds surgical complexity. Xenografts and allografts are commonly used and can perform very well in the right indication, especially when combined with sound surgical technique and membrane stabilization. In many practices, platelet concentrates such as PRF are also used to support soft tissue healing and improve the biologic environment.
The best material is not the most expensive or the most advanced-sounding one. It is the one that fits the defect, the treatment plan, and the biology of healing.
What affects success after grafting?
Surgical technique matters, but so does case selection. A graft needs blood supply, space maintenance, stability, and tension-free soft tissue closure. If the membrane moves, the flap opens, or the site becomes contaminated, the outcome can be compromised.
Patient factors are just as important. Smoking increases the risk of impaired healing. Poor plaque control raises the chance of inflammation. Clenching and uncontrolled systemic disease can complicate recovery. Even anatomy matters – thin soft tissue and severe ridge collapse are simply harder situations than a fresh extraction socket with intact walls.
This is why a proper consultation should feel specific. If every patient is given the same timeline and the same grafting explanation, something is missing.
Is bone grafting painful?
Most patients expect the graft to be much harder than it actually is. With appropriate local anesthesia and careful surgical handling, the procedure is usually well tolerated. Postoperative discomfort varies more by the size of the surgery than by the concept of grafting itself.
A small socket preservation procedure is often easier than a difficult tooth extraction. Larger augmentations can involve more swelling and a longer recovery, especially in the upper jaw when sinus work is involved. Good microsurgical technique, careful flap design, and clear postoperative instructions make a meaningful difference in comfort.
The emotional side matters too. Surgical treatment feels easier when patients understand why each step is being done and what to expect next.
Bone graft before implant placement in the esthetic zone
The front teeth deserve special mention because this is where shortcuts tend to show. In the esthetic zone, the issue is not only implant survival but tissue architecture – the gum line, papillae, and ridge contour. If the facial bone plate is thin or missing, placing an implant without rebuilding support can lead to recession and an artificial-looking result.
That is why treatment in this area often requires a more disciplined sequence. Extraction timing, socket preservation, connective tissue management, provisionalization, and implant positioning all influence the final appearance. A patient may feel impatient about staging, but this is often exactly what protects the esthetic outcome.
Why proper planning matters more than speed
A fast treatment plan is appealing, but speed is not the same as efficiency. The most efficient implant treatment is the one that avoids preventable complications and reduces the likelihood of revision surgery later.
In experienced hands, bone grafting is not an obstacle to implant therapy. It is part of making implant therapy possible in cases where the anatomy is no longer ideal. With modern imaging, prosthetically driven planning, microsurgical protocols, and biologically sound healing timelines, even challenging sites can often be restored predictably.
For patients considering treatment, the real question is not whether grafting adds a step. It is whether that step improves the quality and longevity of the final result. In many cases, it clearly does.
If you have been told you need grafting, ask your surgeon to show you the anatomy, explain the defect, and describe whether the plan is simultaneous or staged. Good implant treatment starts when the plan is clear enough that the surgery no longer feels like guesswork.
Comments (0)