A patient hears they have “not enough bone” and often assumes the conversation is over. In reality, the question is rarely that simple. If you are wondering can bone loss stop implants, the honest clinical answer is sometimes – but very often, it changes the treatment plan rather than ruling treatment out.
Bone loss matters because a dental implant needs stable surrounding bone for initial fixation and long-term support. But modern implant dentistry is not limited to ideal cases. With proper imaging, careful surgical planning, and the right regenerative techniques, many patients with reduced bone volume can still be treated predictably.
Can bone loss stop implants in every case?
No. Bone loss can make implant treatment more complex, but it does not automatically disqualify you.
The key issue is not just the amount of bone. We also evaluate bone width, bone height, density, the position of nearby anatomical structures, bite forces, gum condition, history of infection, smoking, diabetes control, and whether the missing tooth was lost recently or many years ago. Two patients may both be told they have bone loss, yet one can receive an implant immediately and the other needs staged treatment first.
This is why a panoramic X-ray alone is often not enough for decision-making. In implant planning, a CBCT scan gives a three-dimensional view of the jaw and helps determine whether there is enough bone for safe implant placement or whether bone augmentation is needed.
Why bone loss happens after tooth loss
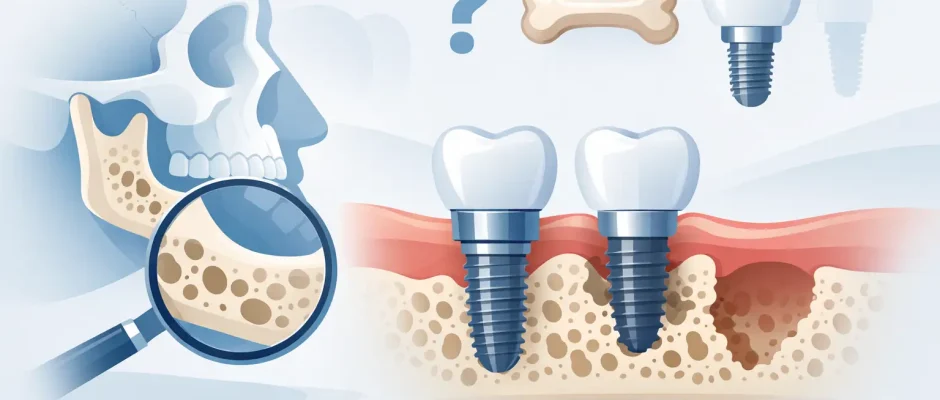
After a tooth is removed or lost, the jawbone in that area no longer receives the same functional load. Over time, the body begins to resorb the bone. This process is often fastest in the first months after extraction, but it can continue for years.
Periodontal disease can accelerate this loss. Chronic infection destroys supporting tissues around teeth, including bone. Trauma, long-term removable dentures, failed root canal treatment with chronic inflammation, and untreated fractures can also contribute. In the upper jaw, the maxillary sinus may expand downward after tooth loss, which reduces available bone height for implants in posterior areas.
That is why early planning matters. The longer a missing tooth is left untreated, the greater the chance that the future implant site will need additional preparation.
When bone loss is a real obstacle
Bone loss becomes a true problem when the implant cannot be placed in a stable, prosthetically correct, and biologically safe position.
If the ridge is too narrow, there may not be enough bone around the implant for long-term support. If bone height is insufficient, the implant may risk encroaching on the sinus in the upper jaw or the inferior alveolar nerve in the lower jaw. If active infection or uncontrolled periodontal disease is present, placing an implant before stabilizing the condition increases the risk of failure.
Severe bone loss also affects esthetics, especially in the front teeth. Even if an implant could technically be inserted, the final gum contour may be compromised without hard and soft tissue reconstruction. In these cases, treatment should not be rushed. A predictable result is more important than a fast one.
What surgeons do when there is not enough bone
In many cases, the answer is not “you cannot have implants,” but “we need to rebuild the site first” or “we need a different protocol.”
Bone grafting
Bone grafting is one of the most common solutions. The goal is to increase ridge width or height so the implant can be placed with better stability and long-term support. Depending on the defect, this may involve particulate graft materials, autogenous bone, membranes, and biologic support such as PRF.
Not every graft is the same. A small contour defect after extraction is very different from a large vertical defect in a long-standing edentulous area. The complexity of the graft, healing time, and predictability depend on the size and shape of the missing bone.
Guided bone regeneration
Guided bone regeneration is often used when the implant site needs localized reconstruction. A graft material is placed and protected with a membrane so the area can heal with better hard tissue formation. This approach can be performed simultaneously with implant placement in selected cases or as a separate stage when the defect is larger.
Sinus lift
In the upper back jaw, reduced bone height is common because of sinus anatomy and post-extraction resorption. A sinus lift creates additional vertical space for implant placement by elevating the sinus membrane and placing graft material beneath it. For many patients, this turns an apparently unsuitable area into a treatable one.
Short, narrow, or angled implants
Sometimes the best solution is not more grafting, but a different implant design or position. Short implants can be effective in selected cases with limited bone height. Narrow implants may help when the ridge is thin, although they are not appropriate for every bite situation. In full-arch rehabilitation, tilted implants can sometimes avoid anatomical limitations and reduce the need for extensive augmentation.
This is where surgical judgment matters. A less invasive option is attractive, but only if it does not compromise stability, load distribution, or long-term maintenance.
Can bone loss stop implants if you want teeth in a day?
It can. Immediate implant placement or immediate loading depends on strict criteria.
Patients often ask for extraction and implant placement in one visit, sometimes with a same-day temporary tooth. This can be an excellent option when infection is controlled, the remaining bone can provide primary stability, and the soft tissue situation is favorable. But significant bone loss may remove that margin of safety.
If the implant cannot achieve enough primary stability, or if the defect is too large to manage predictably in one stage, delaying placement is the safer decision. From the patient perspective, that may feel slower. From the clinical perspective, it is often what protects the final result.
How we decide whether implants are still possible
A proper evaluation is structured, not guesswork. The decision usually includes clinical examination, CBCT analysis, periodontal assessment, and restorative planning before surgery begins.
We do not only ask whether an implant fits into the bone. We ask whether it can be placed in the correct position for the future crown, whether the gum architecture can be supported, whether the patient can maintain hygiene, and whether the risk factors are controlled. A technically placed implant that is poorly positioned or difficult to clean is not a successful treatment plan.
Digital planning and surgical guides add another layer of predictability, especially in reduced bone volume. When anatomy is limited, precision matters even more. A few millimeters can change whether treatment is straightforward, graft-dependent, or unsafe.
The factors that affect success when bone is limited
Bone volume is only one variable. Smoking increases complication rates and impairs healing. Uncontrolled diabetes can negatively affect tissue response. Active gum disease must be treated before implant therapy. Teeth grinding may overload implants and influence the prosthetic design.
Oral hygiene also matters more than many patients expect. An implant can integrate well surgically and still develop inflammatory problems later if plaque control is poor. In patients with previous periodontal disease, maintenance is especially important.
There is also a timing question. In some cases, preserving bone at the time of extraction with socket grafting makes future implant treatment simpler. In others, the site has already healed with atrophy and needs a more advanced reconstruction. Earlier intervention often gives us more options.
What patients should ask at the consultation
If you have been told you have bone loss, ask how severe it is and where it is located. Ask whether the issue is width, height, density, or a combination. Ask if the implant can be placed immediately, after grafting, or only with an alternative full-arch protocol.
You should also ask what the final treatment is aiming to achieve. For some patients, the priority is replacing a single tooth with natural gum contours. For others, it is restoring function in a full arch with the fewest surgeries possible. The right plan depends on the anatomy, but also on the clinical goals.
A careful surgeon should be able to explain the trade-offs clearly. More grafting may improve anatomy and esthetics but increase treatment time, cost, and healing stages. A simplified approach may shorten treatment but require compromises in tissue contour or prosthetic design. Good planning means choosing consciously, not optimistically.
When a second opinion makes sense
If you were told implants are impossible based on a basic X-ray or a very brief consultation, a second opinion is reasonable. This is especially true in cases of posterior maxillary bone loss, narrow ridges, or long-standing missing teeth, where advanced surgical options may still exist.
Complex cases benefit from a surgeon who routinely works with bone deficiency, sinus lift procedures, guided bone regeneration, and digitally planned implant placement. Experience does not change anatomy, but it often changes what can be done safely and predictably.
At Implantolog.co.il, this is often the turning point for anxious patients – moving from a vague “probably not” to a clear plan with defined stages, timelines, and realistic expectations.
Bone loss should be taken seriously, but it should not be interpreted as an automatic dead end. The real question is not only whether there is less bone today, but what can be rebuilt, what can be planned around, and what approach gives you the safest long-term result.
Comments (0)