Dental Implant Nerve Damage Explained
A patient expects some soreness after implant surgery. What they do not expect is a lip that stays numb, a chin that tingles, or an electric-shock sensation when speaking or eating. That is why dental implant nerve damage deserves a clear, practical explanation – not alarmism, and not vague reassurance.
In most properly planned implant cases, nerve injury is avoided. But the risk is real, especially in the lower jaw where the inferior alveolar nerve and the mental nerve run close to common implant sites. The key question is not only whether nerve damage can happen. It is how it happens, how it is prevented, and what should be done if symptoms appear.
What dental implant nerve damage actually means
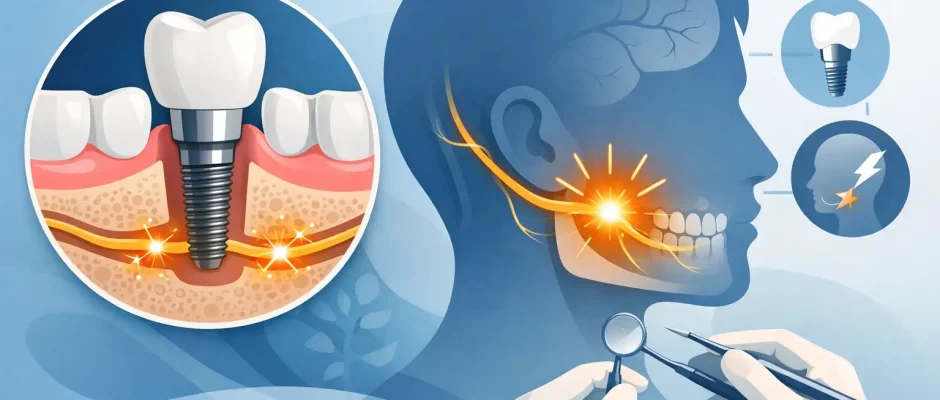
Dental implant nerve damage refers to irritation, compression, stretching, overheating, or direct trauma to a nerve during or around implant placement. The lower jaw is the main area of concern because the inferior alveolar nerve travels inside the mandibular canal and gives sensation to the lower lip, chin, and teeth. Near the premolar area, the mental nerve exits through the mental foramen and can also be affected.
In the upper jaw, nerve injuries related to implants are less common and usually involve smaller sensory branches rather than a major nerve trunk. For most patients, when people talk about implant-related nerve injury, they mean altered sensation in the lower lip or chin after mandibular implant surgery.
The severity can vary. A mild temporary irritation may cause numbness that improves over days or weeks. A more significant injury can lead to persistent altered sensation, burning, pain, or dysesthesia, which is an unpleasant abnormal feeling triggered by light touch or even at rest.
How nerve injuries happen during implant treatment
The simplest explanation is lack of distance between the implant and the nerve. If the implant osteotomy is prepared too deep, or if the implant itself extends into the mandibular canal, the nerve can be compressed or injured. Sometimes the issue is not the implant body but the drilling process, especially if planning was based on limited imaging or anatomical landmarks were misjudged.
Heat is another mechanism. Bone drilling generates temperature, and without proper irrigation and controlled technique, thermal injury can occur. Less often, local anesthetic injection, flap elevation, retraction, or postoperative swelling can contribute to temporary nerve irritation.
There is also a subtler scenario: the anatomy is unusual. The mandibular canal may run higher than expected, the mental foramen may be positioned more coronally, or an anterior loop of the mental nerve may extend farther forward than a standard estimate suggests. This is exactly why routine assumptions are not enough in implant surgery.
Why careful planning matters more than luck
Most serious complications are preventable with correct diagnostics and disciplined execution. A panoramic X-ray can provide orientation, but for lower jaw implant planning near critical anatomy, three-dimensional imaging is often what changes uncertainty into measurable safety.
CBCT allows the surgeon to evaluate bone height, width, angulation, canal position, and anatomical variations. That makes it possible to choose implant length and diameter with an actual safety margin rather than a guess. In more demanding cases, digital planning combined with a surgical guide adds another layer of control by translating the virtual plan into the mouth with high precision.
This is where experience matters. Not because experienced surgeons are immune to complications, but because they are more likely to recognize high-risk anatomy, avoid borderline decisions, and modify the plan when the available bone does not support a safe implant position. Sometimes that means choosing a shorter implant. Sometimes it means changing angulation, staging treatment, or performing bone augmentation instead of forcing an implant into a compromised site.
Symptoms patients should never ignore
Not every unusual feeling after surgery means nerve injury. Local anesthesia can last for several hours, and postoperative swelling can create temporary pressure. Mild transient tingling may resolve without intervention. But there are symptoms that require prompt contact with the surgeon.
Persistent numbness of the lower lip, chin, or gums after the anesthetic should have worn off is the most classic warning sign. Tingling, pins and needles, burning pain, heightened sensitivity, or a painful electric feeling can also indicate nerve involvement. Some patients describe a thick, heavy, or “different” sensation rather than complete numbness.
Timing matters. If altered sensation is noticed immediately after surgery and does not improve as the anesthesia fades, the case should be assessed quickly. Early action can make a meaningful difference.
Diagnosing dental implant nerve damage
The first step is a careful clinical history. When did the altered sensation start? Is it numbness, tingling, pain, or hypersensitivity? Is it stable, improving, or worsening? Which exact area is affected?
Clinical sensory testing helps map the deficit. The surgeon may check light touch, pinprick, two-point discrimination, and response to temperature. Imaging is then used to understand the anatomical relationship between the implant and the nerve. A postoperative CBCT is often the most informative test when direct proximity or canal encroachment is suspected.
The goal is not only to confirm that dental implant nerve damage has occurred. It is to identify the mechanism. Compression by the implant, drilling trauma, hematoma-related pressure, and transient neurapraxia do not all carry the same prognosis or require the same response.
What treatment depends on
Management depends on severity, timing, and the imaging findings. If the implant appears to impinge on the nerve canal, early removal or repositioning may be indicated. This is one of the few situations in implant dentistry where waiting too long can reduce the chance of recovery. If the nerve is under ongoing mechanical pressure, the problem is unlikely to improve on reassurance alone.
If the implant is close but not clearly within the canal, and symptoms are mild or improving, treatment may be more conservative. Anti-inflammatory medication may be used in selected cases. Some clinicians also use neurosensory follow-up over time to document recovery. If symptoms persist, referral to a specialist with experience in microsurgical nerve assessment may be appropriate.
There is no honest single timeline for healing. Some temporary injuries improve within days or weeks. Others take months. A small number can leave permanent sensory changes. That uncertainty is frustrating for patients, but it is part of informed consent and responsible postoperative care.
Can the nerve recover?
Often, yes – but not always completely. A mild compression or stretch injury has a better prognosis than direct penetration or severe trauma. Earlier diagnosis generally improves the chance of recovery, especially if there is something correctable, such as implant compression.
Recovery is also not all-or-nothing. A patient may regain normal protective sensation but still notice slight tingling. Another may lose numbness but develop an unpleasant altered sensation instead. This is why follow-up should focus on function and quality of life, not only on whether “feeling came back.”
How to reduce the risk before surgery
For patients, the practical question is simple: how do you stack the odds in your favor? Start with diagnosis, not speed. If lower jaw implants are being planned without appropriate three-dimensional assessment in an anatomically tight area, that is a reason to ask more questions.
The second issue is planning discipline. A surgeon should be able to explain where the nerve is, what safety distance is being used, whether a guide is useful in your case, and what alternatives exist if the bone height is limited. Good planning is rarely dramatic. It is careful, measured, and a little conservative when anatomy demands it.
Technique matters just as much as imaging. Controlled drilling, proper irrigation, stable angulation, and respect for anatomical limits are not marketing language. They are the everyday details that protect patients.
This is one reason digitally planned, guided surgery can be valuable in selected cases. It does not replace judgment, and it is not necessary for every implant. But when bone is limited or anatomy is close, digital protocols can improve precision and reduce avoidable deviation.
When risk is higher
Not all implant sites carry the same nerve risk. Posterior mandibular implants are typically the most sensitive because of their relationship to the inferior alveolar nerve. Premolar-region surgery requires attention to the mental foramen and any anterior loop. Severe bone resorption can also increase risk because the available bone above the canal is reduced.
Revision cases, immediate implants after extraction, and complex full-arch planning can introduce additional variables. That does not mean these treatments are unsafe. It means they should be approached with a higher level of anatomical planning and surgical control.
For patients traveling for care, this becomes even more relevant. It is worth choosing a surgeon who routinely manages complex implant cases, uses modern imaging and guided protocols when indicated, and has a clear postoperative follow-up process. In a surgical practice focused on predictable implant treatment, including complex cases in Tel Aviv, those details are part of safety, not extras.
A balanced perspective
Nerve injury after implant surgery is uncommon, but it is not trivial. The right response is neither fear nor dismissal. It is respect for anatomy, precise planning, and early action if symptoms suggest a problem.
If you are considering an implant in the lower jaw, ask your surgeon to explain the nerve position, the imaging used, and the specific safety strategy for your case. A good surgical plan should leave you feeling informed, not rushed.
Comments (0)