How Long Do Dental Implants Last Compared to Bridges?
A missing tooth creates a practical decision, not just a cosmetic one: restore it with a bridge now, or undergo implant treatment designed to preserve the jawbone over time. Patients often ask, how long do dental implants last compared to bridges? The short answer is that an implant can support a restoration for decades, while a conventional bridge commonly requires replacement sooner. But the useful answer depends on your gums, bone, bite, hygiene, and the quality of planning before treatment begins.
How Long Do Dental Implants Last Compared to Bridges?
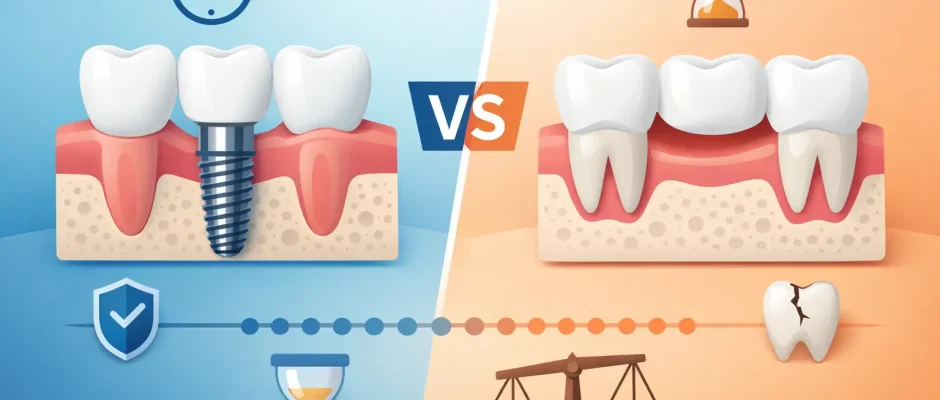
A dental implant is a titanium fixture placed in the jawbone to replace the tooth root. Once it has integrated with the bone, it supports an abutment and a crown. The implant fixture itself may last a lifetime. The visible crown is a separate component, however, and usually needs replacement after about 10 to 15 years because of normal wear, chipping, changes at the gum line, or damage from heavy biting forces.
A conventional dental bridge is usually expected to last about 7 to 15 years. Some bridges remain functional for 20 years or longer, especially when they are well designed and the supporting teeth and gums stay healthy. Still, a bridge depends on neighboring natural teeth. If decay develops around a crown margin, a supporting tooth cracks, or gum disease causes bone loss, the entire bridge may need repair or replacement.
For this reason, implants generally offer the longer-term solution when a patient is medically suitable for surgery and has enough bone or can safely undergo bone augmentation. A bridge can still be an excellent restoration in the right clinical situation. Longevity is not the only factor that matters.
Why an Implant Can Last Longer
The central advantage of an implant is that it functions independently. It does not require the dentist to reduce healthy enamel on the teeth next to the gap, and it does not connect those teeth into one unit. This makes daily cleaning more straightforward and avoids placing bridge-related stress on adjacent teeth.
Implants also transmit chewing forces into the jawbone. That stimulation helps limit the gradual bone resorption that follows tooth loss. A bridge restores the visible tooth and chewing surface, but it cannot replace root-level stimulation beneath the missing tooth area. Over years, the ridge under a bridge may become narrower or lower, which can affect appearance and make a future implant more complex.
That said, an implant is not indestructible. The titanium fixture does not decay, but the tissues around it can become inflamed. Mucositis is inflammation of the soft tissue around an implant. If untreated, it can progress to peri-implantitis, which involves bone loss around the implant and can threaten its stability. Professional maintenance and precise home care remain necessary for the life of the restoration.
What Shortens the Life of an Implant?
An implant can fail early, before it integrates with bone, or later, after years of function. Early complications are uncommon with proper diagnosis and surgical protocol, but risk rises when the implant is placed without adequate bone volume, stable positioning, or control of infection.
Late complications are more often linked to inflammation, excessive bite forces, and difficulty cleaning around the restoration. Smoking is a significant risk factor because it can impair healing and increase the likelihood of peri-implant disease. Poorly controlled diabetes, untreated periodontal disease, and inconsistent recall visits also deserve attention before treatment begins.
Bruxism, or habitual grinding and clenching, affects both implants and bridges. An implant does not have the same natural shock-absorbing ligament as a tooth. In patients with a powerful bite, careful prosthetic design, bite adjustment, and a protective night guard may be essential. These details are not extras. They are part of protecting the investment in treatment.
In complex cases, three-dimensional imaging and digital planning help the surgeon evaluate bone width, bone height, anatomical structures, and the future position of the crown. When indicated, a surgical guide can improve the accuracy of implant placement. If bone is deficient, procedures such as guided bone regeneration or sinus lift surgery may create the conditions needed for a stable, correctly positioned implant rather than accepting a compromised placement.
What Shortens the Life of a Bridge?
The weak point of a bridge is usually not the ceramic itself. It is the supporting teeth. A bridge may fail when bacteria enter at the edge of a crown and cause recurrent decay beneath it. This can be difficult for a patient to notice at an early stage, particularly when a bridge is older or the margin lies close to the gum line.
A root canal-treated supporting tooth may be more vulnerable to fracture, depending on how much natural structure remains. If one anchor tooth fails, replacing the bridge may require treatment of multiple teeth, extraction, or a new implant-based plan. In other words, a bridge can be durable, but its long-term prognosis is linked to the prognosis of every tooth that supports it.
Cleaning also requires technique. A patient needs to clean beneath the artificial tooth using floss threaders, super floss, or an interdental brush appropriate for the space. If plaque accumulates under the bridge, gum inflammation and decay around the abutment teeth can follow. This does not mean bridges are difficult to maintain, but it does mean they need daily attention beyond ordinary brushing.
When a Bridge May Be the Better Choice
Choosing a bridge is not necessarily choosing an inferior result. It may be a sensible option when the neighboring teeth already have large fillings or crowns and would benefit from coverage anyway. A bridge can also be appropriate when surgery is medically contraindicated, when a patient prefers a shorter treatment timeline, or when an implant site requires extensive reconstruction that the patient does not wish to pursue.
An adhesive resin-bonded bridge, often used in the front of the mouth, may be especially conservative when adjacent teeth are intact. It usually has a different longevity profile from a conventional bridge and may occasionally need rebonding, but it can preserve more healthy tooth structure.
There are also situations where an implant should be delayed. Active gum disease must be stabilized first. A recent extraction site may need time to heal, unless immediate implant placement is appropriate and can be performed predictably. For young patients whose jaw growth is not complete, an implant is generally postponed.
The Cost Question Should Include the Next 15 Years
A bridge often has a lower initial cost and can be completed faster than implant treatment. Implant treatment may involve extraction, grafting, healing time, implant placement, and the final crown. Looking only at the first invoice, a bridge can appear simpler.
However, the long-term comparison should include the possibility of bridge replacement and treatment of supporting teeth. If a bridge must be replaced several times over a lifetime, or if an abutment tooth is eventually lost, the original lower cost may become less decisive. Conversely, an implant is not automatically the best financial choice if a patient cannot commit to maintenance or has health factors that make its prognosis uncertain.
A thoughtful treatment plan should identify what is being preserved, what risks are present, and what future treatment might be required. This is particularly valuable in cases involving bone loss, multiple missing teeth, or a history of periodontal disease.
How to Help Either Restoration Last
The most durable restoration is supported by healthy tissues and regular care. Brush carefully twice a day, clean between teeth and around the restoration every day, and attend professional examinations and hygiene visits at the interval recommended for your risk level. X-rays may be needed periodically to assess the bone around implants or the supporting teeth beneath a bridge.
Report bleeding, swelling, a bad taste, looseness, pain when chewing, or a change in how your teeth meet. These symptoms do not always mean failure, but early evaluation can prevent a minor issue from becoming a more involved treatment.
For patients considering treatment in Tel Aviv, the decision should begin with a clinical examination, periodontal assessment, and three-dimensional diagnostic planning when an implant is under consideration. The goal is not to sell the longest-lasting option in the abstract. It is to select the restoration that can be placed safely, cleaned reliably, and maintained predictably in your specific mouth.
A bridge can serve well for many years, and a well-planned implant may serve for decades. The better choice is the one that protects your remaining teeth, respects your biology, and gives you a realistic plan for care long after the procedure is complete.
Comments (0)