When patients ask about all-on-4 vs all-on-6 implants, they are usually not asking about numbers alone. They are asking a more practical question: which solution will be more stable, safer, and more predictable for my mouth over time? That distinction matters, because the right choice is not the one with more implants on paper. It is the one that matches your bone anatomy, bite forces, smile line, medical history, and the quality of the treatment plan.
Both concepts are designed to restore a full arch of teeth on a fixed prosthesis. Both can work very well in the right case. But they are not interchangeable, and treating them as if they are can lead to unnecessary compromises.
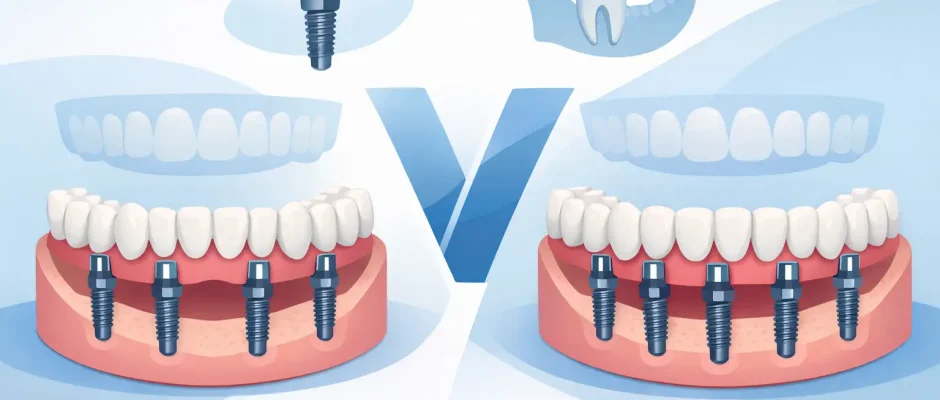
All-on-4 vs all-on-6 implants: what is the real difference?
In simple terms, All-on-4 uses four implants to support a full-arch bridge, while All-on-6 uses six. The difference sounds small, but clinically it changes load distribution, biomechanical reserve, and sometimes the need for additional surgical preparation.
With All-on-4, the two posterior implants are often angled to use available bone and avoid anatomical structures such as the maxillary sinus or the inferior alveolar nerve. This makes it possible to deliver a fixed solution even in patients with reduced bone volume, often without major grafting. That is one reason the protocol became so popular.
With All-on-6, there are two additional implants, usually allowing support to be spread more evenly across the arch. In many patients, this improves biomechanical balance and reduces the load carried by each implant. It can be especially useful in the upper jaw, where bone quality is often softer and chewing forces may be less forgiving.
The key point is this: more implants do not automatically mean a better result. But in the right anatomy, six implants can provide a wider safety margin.
When All-on-4 makes sense
All-on-4 is often a strong option when bone volume is limited and the goal is to avoid more extensive grafting. It can also be appropriate when the patient wants a fixed restoration with fewer surgical steps, a shorter overall treatment path, or a lower financial threshold.
This does not mean it is a “budget version” of full-arch treatment. In experienced hands, with proper digital planning and careful prosthetic design, All-on-4 can function very well for many years. What matters is not the marketing label but whether the implants can be placed in prosthetically correct positions with good primary stability.
It tends to work best when the arch form, bone availability, and bite relationship allow a controlled prosthetic cantilever. If that cantilever becomes too long, the bridge may be exposed to higher bending forces, and that changes the long-term picture.
When All-on-6 is the better choice
All-on-6 is often preferred when anatomy allows placement of six well-positioned implants without unnecessary risk. The extra implants can reduce stress on the system and may allow a shorter cantilever or, in some cases, no cantilever at all. That usually improves mechanical predictability.
This matters most in patients with strong bite forces, signs of clenching or grinding, larger arches, or cases where the upper jaw has lower bone density. It can also be a smart choice when the treatment goal is to build in more redundancy. If one implant develops a problem years later, a six-implant restoration may offer more flexibility than a four-implant design.
That said, All-on-6 is not always worth pursuing at any cost. If placing six implants requires aggressive grafting, poor implant positioning, or compromises near anatomical structures, then the theoretical advantage may disappear.
Bone volume and anatomy often decide more than preference
One of the biggest mistakes in full-arch treatment is choosing a concept before analyzing the anatomy. The amount and quality of available bone, the position of the sinuses, the shape of the jaw, and the restorative space all affect the decision.
In the lower jaw, dense bone often allows excellent fixation, and either concept may be possible depending on the clinical situation. In the upper jaw, the decision is usually more demanding. Bone is often softer, posterior support may be limited by the sinus, and implant distribution becomes especially important.
This is why CBCT-based planning is central to a safe decision. A full-arch case should not be selected from a panoramic image alone or from a price list. Digital planning helps determine whether implants can be placed where the future teeth actually need support. If guided surgery is used appropriately, it can improve precision and reduce surprises during the procedure.
All-on-4 vs all-on-6 implants and immediate loading
Many patients also want to know whether they can receive fixed temporary teeth right after surgery. In both All-on-4 and All-on-6 cases, immediate loading may be possible, but only when implant stability is high enough and the bite can be controlled properly.
Immediate loading is not a gift that comes automatically with the protocol. It is a clinical decision. If the implants are stable, the occlusion is well managed, and the temporary bridge is designed correctly, immediate function can be both comfortable and predictable. If those conditions are not met, forcing a same-day fixed solution can increase risk.
In practice, six implants may offer more flexibility for immediate loading because the load is distributed over more supports. Still, a well-executed All-on-4 can also be loaded immediately with very good outcomes. The deciding factor is case quality, not just implant count.
Cost, maintenance, and long-term value
Cost is a reasonable part of this conversation. All-on-6 is usually more expensive than All-on-4 because it involves two additional implants and may require more surgical and prosthetic work. But price alone should not drive the choice.
A lower initial fee can become more expensive if the case is underengineered for the patient’s functional demands. On the other hand, adding implants simply because “more is better” can also be unnecessary. The goal is proportional treatment – enough support for long-term function, no less and no more.
Maintenance should also be part of the discussion. Full-arch restorations require hygiene access, professional follow-up, and periodic checks of screws, prosthetic components, and soft tissue health. A well-designed bridge on four implants can be easier to clean than a poorly contoured bridge on six. Prosthetic design matters as much as surgical planning.
Common situations where the answer is “it depends”
A patient with advanced tooth loss and moderate posterior maxillary atrophy may be an excellent All-on-4 candidate if angled implants can achieve strong anchorage and support a controlled bridge design. Another patient with a wide upper arch, parafunction, and enough bone for six axial or near-axial implants may clearly benefit from All-on-6.
A younger patient who wants maximum long-term reserve may lean toward six implants if anatomy supports it. An older patient with medical limitations may benefit from a simpler, shorter protocol with fewer surgical demands. Neither choice is inherently superior outside the clinical context.
This is where experience matters. Full-arch implant treatment is not just implant placement. It is prosthetically driven surgery. The surgeon must understand force distribution, soft tissue management, restorative space, phonetics, and the patient’s ability to maintain hygiene over time.
What to ask before choosing
Before committing to treatment, ask how the plan was made. Was it based on a CBCT scan and digital prosthetic planning? Will the future bridge have a long cantilever? Is immediate loading realistic in your case or just being promised? What is the contingency plan if one implant does not reach ideal stability on the day of surgery?
You should also ask about the final prosthesis, not only the surgery. The materials, fit, cleansability, and bite scheme will influence your outcome every day after healing is complete. A technically correct surgery followed by a compromised prosthetic phase is still a compromised result.
In complex cases, especially with bone loss or previous dental failures, a conservative and well-reasoned plan is usually better than an aggressive promise. At Implantolog.co.il, this kind of decision is approached through diagnostics first, then a step-by-step plan built around anatomy, function, and safety rather than a one-size-fits-all protocol.
If you are comparing all-on-4 vs all-on-6 implants, the best next step is not to look for the “best system.” It is to find out what your jaw can support predictably, what your bite will demand over the years, and what treatment plan gives you the most stable result with the fewest unnecessary compromises. That is the kind of answer worth building a smile on.
Comments (0)